

Introduction: Treatment of relapsed and refractory multiple myeloma (RRMM) continues to evolve as most patients are lenalidomide (LEN) refractory at the time of first relapse with its widespread use in both induction and maintenance therapy. Pomalidomide, bortezomib and dexamethasone in RRMM has demonstrated significant activity and improvement in progression-free survival in LEN-refractory patients (Richardson et al Lancet Oncol 2019 Jun;20(6):781-794). Ixazomib is a novel oral proteasome inhibitor (PI) that is currently approved in combination with LEN and dexamethasone in RRMM. Ixazomib is administered on a once weekly schedule and its oral route of administration is particularly attractive, not least in the context of the current COVID-19 pandemic. Twice weekly dosing of ixazomib has been studied in combination with LEN demonstrating promising activity in NDMM (Richardson et al, Br J Haematol. 2018 Jul;182(2):231-244). Moreover, safety and efficacy has been shown in RRMM as twice weekly monotherapy on this schedule (Richardson et al, Blood 2014 Aug 14;124(7):1038-46). We hypothesized that a twice weekly ixazomib schedule in combination with pomalidomide and dexamethasone will lead to enhanced efficacy and comparable safety in RRMM.
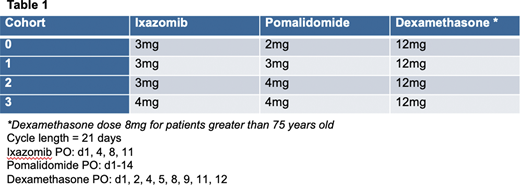
Methods: This is a phase I/II multicenter, single-arm, open label study evaluating the combination of twice weekly ixazomib with pomalidomide and dexamethasone in RRMM. Primary objective for phase I portion is to determine safety and the maximum tolerated dose (MTD) of this combination using a standard 3+3 dose escalation design. Ixazomib is studied at doses of 3mg or 4mg on days 1, 4, 8, 11, pomalidomide at a dose of 2mg, 3mg and 4mg on days 1-14 and dexamethasone is administered at a dose of 12mg on days 1, 2, 4, 5, 8, 9, 11, 12 (8mg for patients > 75 years old) on a 21 day cycle (Table 1). Patients were included if they received 2 prior lines of therapy, but 1 prior line was allowed if first line treatment included a PI and an immunomodulatory agent and disease relapse occurred within 60 days of last therapy. Patients who received prior ixazomib were excluded.
Results: At the time of data cutoff, 12 patients have been enrolled across cohorts 0, 1 and 2 and enrollment in the final cohort 3 is ongoing. Median age at the time of enrollment was 70 years old with slight male predominance (58%). ISS stage at diagnosis was II or greater in 75% of patients and 9 out of 12 (75%) patients had high-risk FISH as follows: del 17p (17%), gain 1q (50%), and t(4;14) (8%). Median prior lines of therapy was 2 (range 1-3) with 100% of patients having prior treatment with lenalidomide and 92% with prior bortezomib. Forty-two percent of patients had a prior autologous stem cell transplant.
Most common treatment-related toxicities were mainly low grade and included neutropenia (58%), hyperglycemia (42%), fatigue (33%), anemia (25%), thrombocytopenia (25%), and rash (25%). Grade 3 or greater toxicities included neutropenia (17%), anemia (8%), bacterial lung infection (8%), and atrial fibrillation (8%). There was 1 dose limiting toxicity (DLT) in cohort 2 due to lung infection necessitating a delay in initiation of cycle 2 and no further DLTs have been noted. Dose reductions occurred in 4 patients and predominantly involved dexamethasone due to weight gain, insomnia, atrial fibrillation and fatigue. There have been no discontinuations due to toxicity and no treatment related mortality at the time of data cutoff. In response evaluable patients, 5 out of 12 patients have demonstrated a partial response or better (42%), with 1 very good partial response (VGPR) and all patients at least achieving stable disease.
Conclusions: Twice weekly ixazomib in combination with pomalidomide and dexamethasone is a generally well-tolerated regimen with promising early activity in a high-risk RRMM cohort. Maximal tolerated dose and recommend phase II dose has not yet been reached and this study continues to accrue robustly, reflecting in part the convenience and safety of an all oral approach in the current era of COVID-19. Moreover, the ability to perform remote laboratory testing, telemedicine visits and to send medications directly to patients has been an additional value-add to this trial. Updated data will be presented at the meeting.
Nadeem:Sanofi: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Adaptive: Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: TRAVEL, ACCOMMODATIONS, EXPENSES; Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees, Other: TRAVEL, ACCOMMODATIONS, EXPENSES. Mo:Celgene: Membership on an entity's Board of Directors or advisory committees. Barth:Sanofi: Membership on an entity's Board of Directors or advisory committees. Sanchorawala:Takeda: Research Funding; Celgene: Research Funding; Prothena: Research Funding; Caelum: Research Funding; Oncopeptide: Research Funding; Regeneron: Other: advisory board; Caleum: Other: advisory board; Proclara: Other: advisory board; Abbvie: Other: advisory board; UpToDate: Patents & Royalties; Janssen: Research Funding. Munshi:BMS: Consultancy; OncoPep: Consultancy, Current equity holder in private company, Membership on an entity's Board of Directors or advisory committees, Patents & Royalties; C4: Current equity holder in private company; Janssen: Consultancy; Adaptive: Consultancy; Legend: Consultancy; Amgen: Consultancy; AbbVie: Consultancy; Karyopharm: Consultancy; Takeda: Consultancy. Ghobrial:Celgene: Consultancy, Honoraria; GlaxoSmithKline: Consultancy; Genentech: Consultancy; Novartis: Consultancy; Noxxon Pharma: Consultancy; Adaptive Biotechnologies: Consultancy, Honoraria; Sanofi: Consultancy, Honoraria; Cellectar: Honoraria; Karyopharm Therapeutics: Consultancy, Honoraria; GNS Healthcare: Consultancy; Janssen: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; AbbVie: Consultancy; Takeda: Consultancy, Honoraria; Bristol-Myers Squibb: Consultancy, Honoraria. Anderson:Oncopep and C4 Therapeutics.: Other: Scientific Founder of Oncopep and C4 Therapeutics.; Bristol Myers Squibb: Membership on an entity's Board of Directors or advisory committees; Sanofi-Aventis: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; Gilead: Membership on an entity's Board of Directors or advisory committees; Millenium-Takeda: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees. Richardson:Celgene/BMS, Oncopeptides, Takeda, Karyopharm: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal